In the 1980s and 1990s, trials showed that giving radiation to the chest wall and nearby lymph nodes after mastectomy helped women with early-stage breast cancer that had spread to their lymph nodes live longer.
These studies, Danish 82b and 82c trials and the British Columbia trial, found that radiation lowered the chance of the cancer coming back in the chest area by about 17-27% and improved overall survival by 8–9% at 10 years.
A later 2014 meta-analysis of prior randomized trials by the Early Breast Cancer Trialists’ Collaborative Group confirmed these results, showing fewer recurrences and better 20-year breast cancer–specific survival for people with one to three positive lymph nodes.
But these earlier studies were done before today’s treatment—before the routine use of taxanes, HER2-targeted therapy, and longer endocrine therapy—leaving uncertainty about whether adding radiation to treatment still provides meaningful benefit.
The Selective Use of Postoperative Radiotherapy after Mastectomy (SUPREMO) trial was designed to answer that question.
The large, international, phase 3 randomized controlled SUPREMO trial asked whether women with “intermediate-risk” early breast cancer truly need routine chest wall radiation after mastectomy when they have already received modern systemic therapy. Results were published on November 5, 2025 in the New England Journal of Medicine.
“Intermediate risk” in this trial was defined as:
A total of 1,679 patients were randomly assigned to receive chest-wall radiation or no radiation. All had undergone mastectomy, axillary surgery, and contemporary systemic treatments.
After about 10 years of follow-up, the results showed no difference in overall survival:
The hazard ratio for death was 1.04 with a 95% Confidence Interval = 0.82–1.30; P = 0.80.
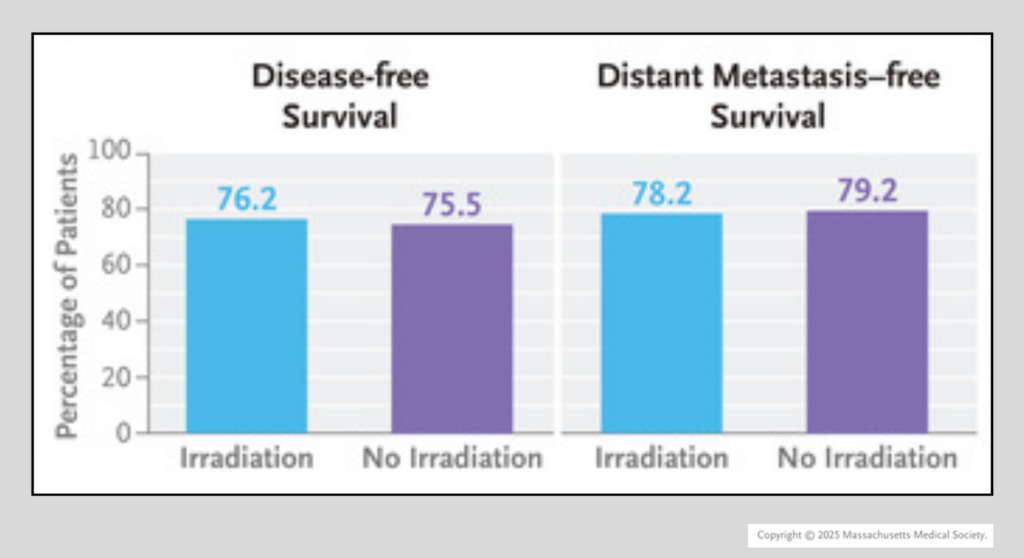
Rates of disease-free and distant metastasis-free survival were also almost the same between the two groups. Local chest-wall recurrence was uncommon in both (1.1% with radiation vs. 2.5% without radiation).
The findings indicate that, with more effective modern breast cancer treatments, adding routine chest-wall radiation for intermediate-risk breast cancer after mastectomy does not improve long-term survival.
For patients, these findings are reassuring, showing excellent long-term outcomes are possible without adding radiation in many intermediate-risk cases—helping people avoid the unnecessary side effects, long-term heart and lung exposure, and added fatigue from treatment.
Radiation is not risk-free: it can cause skin and tissue damage, heart disease, lung inflammation, lymphedema, and, in some cases, secondary cancers. For some patients, these complications can be serious or even result in death years after treatment.
For advocates, the SUPREMO trial is an important example of why we need strong, carefully designed randomized trials to guide smarter, less aggressive care when the evidence supports it—something NBCC commends.
It highlights the importance of continuing to test de-escalation strategies: studies that ask not only “what can we add?” but also “what can we safely remove?”




